Introduction
Chimeric antigen receptor (CAR) therapies involve the use of engineered receptors capable of redirecting immune cells to recognize and destroy cancer cells expressing a specific antigen. Currently, CAR-T cells, T cells equipped with CAR, dominate the field of CAR therapy. Since 2017, over 700 clinical trials involving CAR-T therapy have been registered and the U.S. Food and Drug Administration (FDA) has approved six CAR-T therapies for the treatment of leukemia, lymphomas, and multiple myeloma (Fig. 1) [1]. However, despite its clinical significance, several factors contribute to the limitations of CAR-T therapy. First, as collecting T cells is costly and time-consuming, this may not be feasible for patients already suffering from a compromised immune system. Second, CAR-T therapies mainly focus on treating hematological malignancies, having limited effectiveness in treating solid tumors. Third, CAR-T cells struggle to penetrate the tumor microenvironment (TME), which can hinder their therapeutic function. To overcome these limitations, promising CAR designs have emerged for multi-target CAR-T alongside novel therapies that utilize other immune cell types such as CAR-Natural killer (NK) and CAR-Macrophage (M) cells.
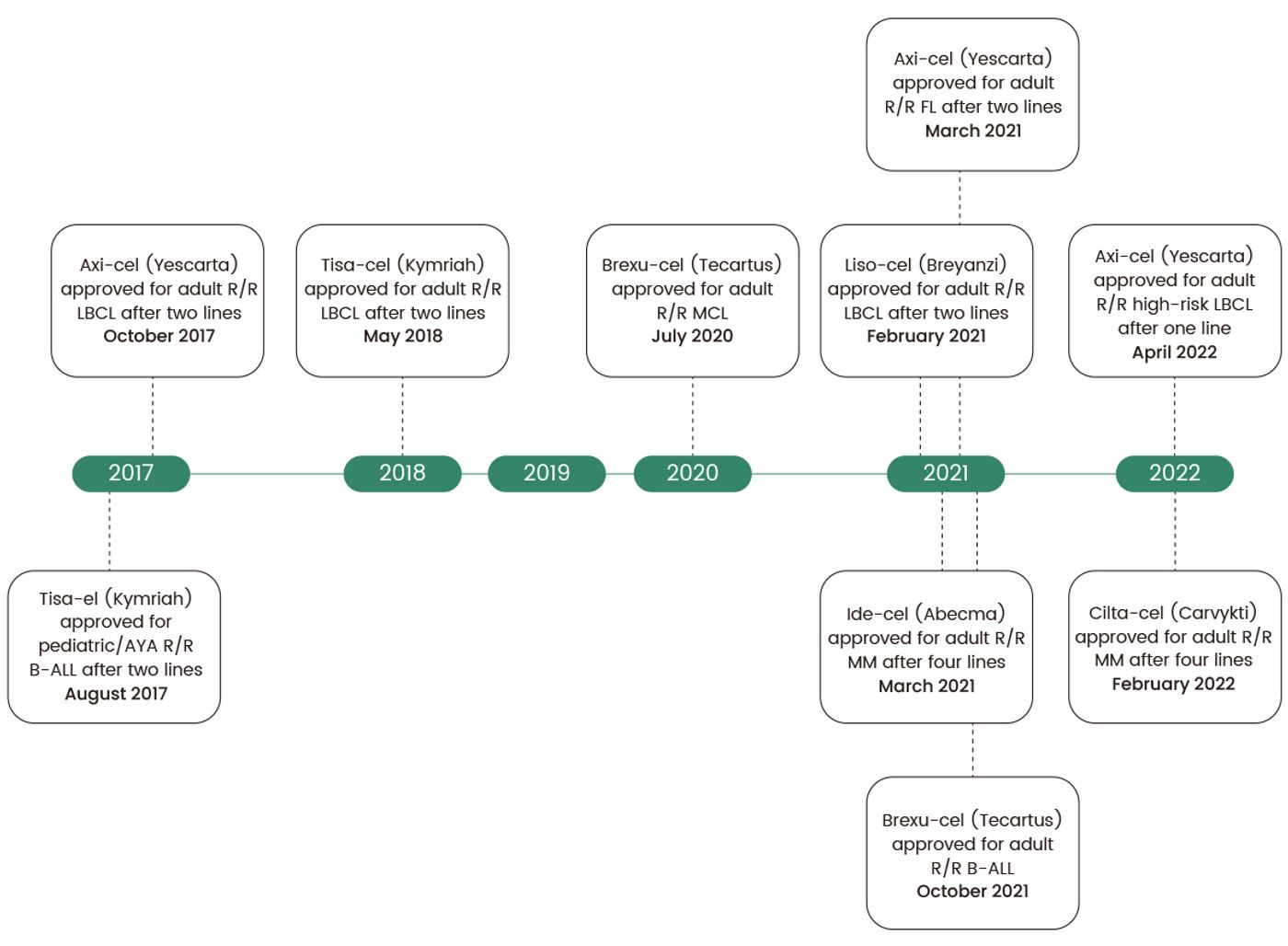
Figure 1. Timeline of CAR-T FDA approvals in the US. B-ALL, B cell acute lymphoblastic leukemia; LBCL, large B cell lymphoma; MCL, mantle cell lymphoma; MM, multiple myeloma; R/R, relapsed/refractorySource: adapted from Maakaron, J, et al. 2022[1]
CAR Molecule Design
CAR is a modified fusion protein derived from the T cell receptor comprising an antigen binding domain and various intracellular signaling domains. The CAR molecule is crucial for therapeutic success as it targets CAR-T cells to attack cancer cells. To be effective, the CAR molecule must have several essential features such as high specificity for the target antigen to ensure that CAR-T cells only attack cancer cells and not healthy ones. Additionally, it should efficiently activate CAR-T cells to ensure a robust immune response, and minimize off-target effects to limit the risk of unintended damage to healthy tissues. Thus, extensive research efforts have focused on optimizing the CAR molecule's efficiency, specificity, and safety, making CAR-T cell therapy a more effective and reliable treatment option for cancer patients.
CARs comprise three major components: an extracellular domain, a transmembrane domain, and an intracellular signaling domain. The extracellular domain includes the signal peptide and the antigen-recognition domain, composed of a single-chain fragment variant (scFV). The transmembrane domain is usually an alpha helix that spans the cell membrane, essential for maintaining the receptor's surface expression and stability. The intracellular domain undergoes conformational changes upon antigen binding to recruit and phosphorylate downstream signaling proteins. Although it can include multiple functional units, the T cell co-receptor CD3ζ's intracellular domain is the primary component of most CARs[2]. It includes three immunoreceptor tyrosine-based activation motifs (ITAMs), which are crucial for signal transduction(Fig. 2A).[3]
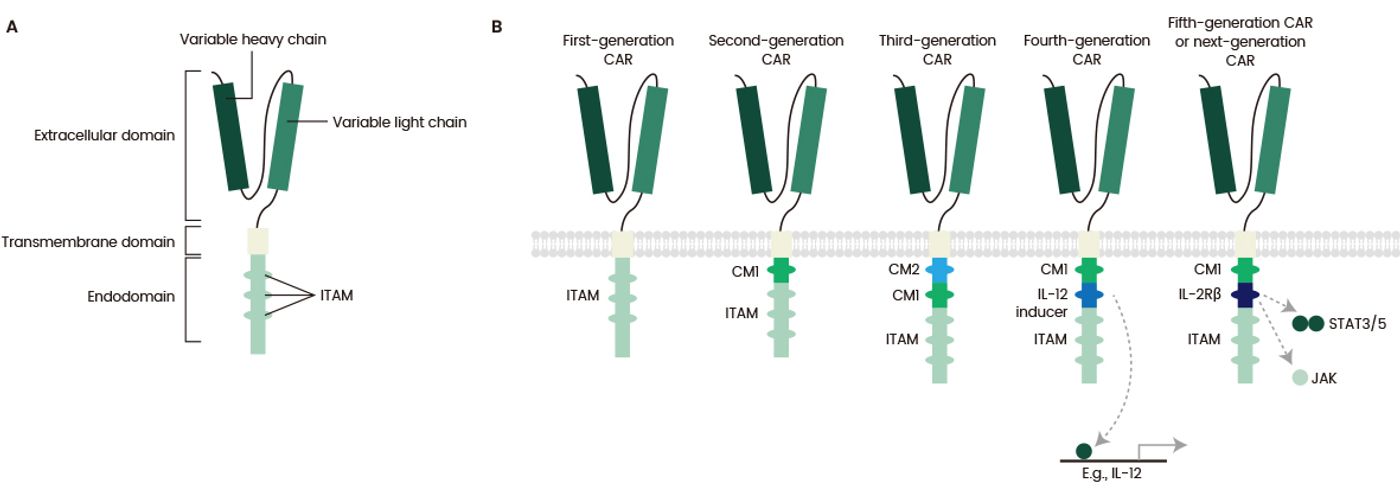
Figure 2. Structure of different chimeric antigen receptor (CAR) generations.
Source:adapted from Tokarew, N, et al. 2019[3]
There are five generations of CARs, with different structure, and composition. The first contained only a CD3ζ intracellular domain, which resulted in low cytotoxicity and proliferation[3]. The second generation added a costimulatory domain to enhance T cell proliferation and cytotoxicity, and the third included an additional costimulatory domain[3]. The fourth generation, known as TRUCKs, included a protein constitutively or inducibly expressed upon CAR activation such as IL-12[3]. The fifth generation, currently under development, contains a truncated cytoplasmic IL-2 receptor β-chain domain with a binding site for the transcription factor STAT3, providing all three synergistic signals required for full T cell activation and proliferation (Fig. 2B).[3]
CAR-Natural Killer (NK)
Natural killer (NK) cells are innate lymphoid cells that can detect and eliminate virus-infected and tumor cells. Over the past two decades, CAR-NK cells have been successfully applied as immunotherapy for advanced-stage leukemia[4].New strategies to enhance NK cell potency and persistence have been developed using co-stimulatory signaling, checkpoint inhibition, and cytokine armors, which redirect NK cell specificity to the tumor through CAR or engager molecules. The promising results of the first generation of CAR-NK cell therapies have sparked continued innovation in the field, such as the development of genetically modified CAR-NK cells, which can kill tumor cells both in CAR-dependent and CAR-independent ways. Compared to traditional CAR-T cells, both CAR-NK cells and unmodified NK cells have safety advantages, such as reduced risks of graft-versus-host disease and alloreactivity[2]. Therefore, they are ideal for immune cell sourcing from sources other than autologous cells, such as NK92 cells, peripheral blood mononuclear cells (PBMCs), umbilical cord blood (UCB), and induced pluripotent stem cells (iPSCs). Unlike T cells, NK cells produce different cytokines, such as GM-CSF, IL-3, and TNF-α, decreasing the incidence and severity of inflammatory cytokine release syndrome and neurological toxicity. In addition, the limited lifespan of CAR-NK cells reduces the risk of cell toxicity.
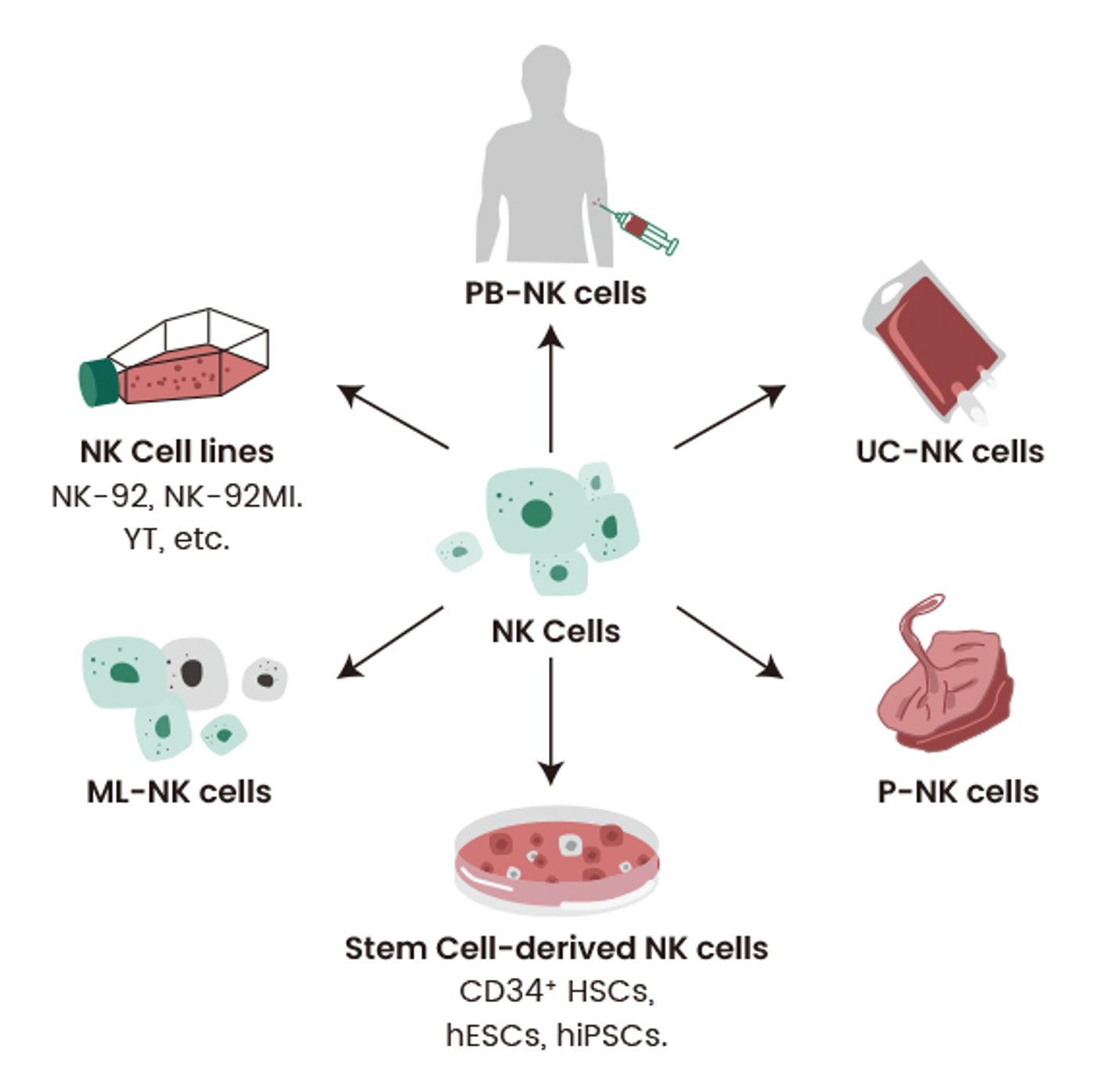
Figure3. Various sources of NK cells. Source: adapted from Zhang L, et al. 2022[5]
According to clinicaltrials.gov, there are currently 26 ongoing clinical trials on CAR-NK targeting of specific antigens in multiple myeloma (CD33, CLL1 and BCMA), acute myeloid leukemia (CD123 and NKG2D), relapsed Bcell non-Hodgkin lymphoma (CD19 and CD70), solid tumors (PD1, CTLA4, Lag3, and 5T4), small cell lung cancer (DLL3), prostate cancer (PSMA), and head and neck cancer (PD-L1)[6]. However, CAR-NK therapies are not yet FDA-approved.
CAR-NK and CAR-T therapies share common challenges such as on-target/off-tumor toxicity, where the CAR-modified cells attack not only the tumor, but also healthy tissues expressing the targeted antigen. Another challenge is the potential for antigen loss or downregulation, leading to treatment failure. Additionally, both therapies face difficulties in targeting solid tumors due to the immunosuppressive TME. However, CAR-NK has several advantages over CAR-T due to its potential for off-the-shelf use, lower risk of cytokine release syndrome (CRS), and ability to target a wider range of tumors due to the lack of major histocompatibility complex restrictions[2,4]. Nonetheless, CAR-NKs exhibit lower potency and persistence than CAR-T cells, which may limit their efficacy against certain cancers. In addition, although the shorter half-life of NK cells can reduce the risk of on-target/off-tumor toxicity to normal cells, it can contribute to poor cytotoxicity in an immunosuppressive TME.
Generating sufficient NK cells is essential for adoptive immunotherapy and cytokines such as IL-2, IL-7, IL-12, IL-15, and IL-21are critical for in vivo growth and survival of NK cells. Sino Biological has successfully developed high-purity, high-activity GMP- grade cytokines to aid in the development of human adoptive immunotherapies.
CAR-M
In contrast to T and NK cells, macrophages possess the ability to infiltrate and persist within tumors. They also exhibit a distinct mechanism of tumor cell killing: phagocytosis[7]. CAR-M and the more recent CAR-M derived from induced pluripotent stem cells (CAR-iMac) are emerging alternatives to conventional CAR-T therapy.
The core components of CAR-M are similar to CAR-T, including an extracellular domain that provides specific recognition via a single-chain variable fragment (scFv), such as CD19 or HER2, a hinge domain, a transmembrane domain (mainly CD8), and an intracellular domain for dedicated downstream signaling, such as CD3z and FcgR.[7] (Fig. 4)
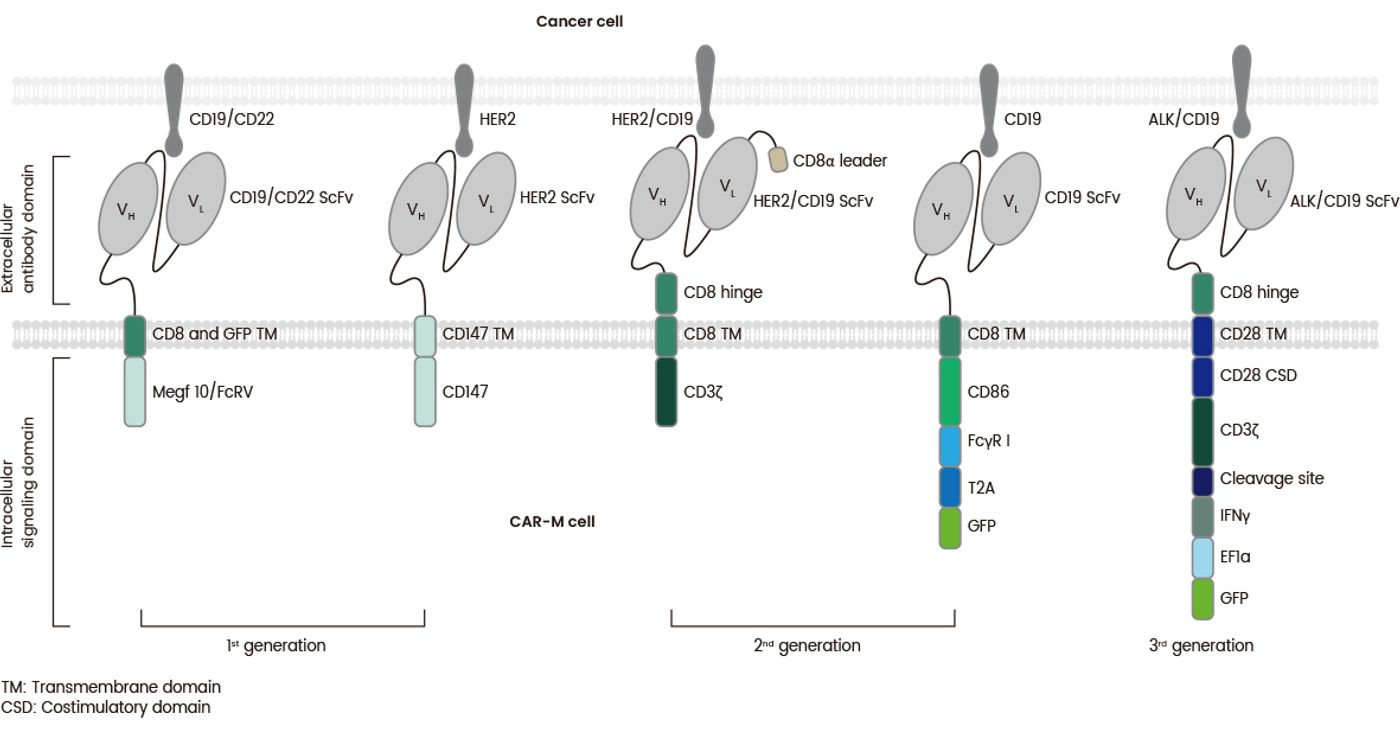
Figure 4. The structures of various generations of CAR-Ms which differ in their intracellular domain. Source: adapted from Wang Sh, et al. 2022[7]
Similar to other CAR-based immunotherapies, CAR-M faces challenges from antigen loss and cytokine toxicity. However, CAR-M has several advantages over CAR-T and CAR-NK, such as superior immune cell trafficking, TME infiltration, and the ability to overcome immunosuppressive TMEs[8,9].Tumor-associated macrophages (TAMs) are particularly abundant in tumors and can efficiently migrate to tumor sites. Studies have revealed that hypoxia-induced tumor cells and stroma secrete chemokines such as CCL2, CCL12, M-CSF, and growth factor VEGFA which correlates with macrophage accumulation[2]. However, CAR-M therapy is still a novel approach, and its research primarily preclinical. A major challenge of macrophage-based therapies is balancing macrophage expansion with therapeutic efficacy. Although iPSCs could serve to generate macrophages, offering a potential solution for efficient macrophage production, this approach is still under development.
Future Outlook
The field of CAR-T therapy has been revolutionary and the most promising cell therapy for hematological tumors as demonstrated by multiple FDA approvals. Ongoing research aims at overcoming the limitations associated with CAR-T therapy and exploring alternative CAR-based therapies such as CAR-NK and CAR-M. While novel strategies for dendritic cells and B cells have been introduced as well, their therapeutic potential requires further investigation.
Moreover, innovative approaches such as the development of multi-target CAR-Ts have emerged to broaden antigen coverage, with recent strategies targeting ≥2 antigens. Multi-target CAR-T cells have been shown to improve anti-tumor efficacy, CAR-T cell persistence and specificity, prevent tumor escape, and decrease the risk of severe CRS[10]. In addition, numerous studies using dual-target combinations and even trivalent CAR-T cells are currently underway. However, the efficacy of novel CAR-based cell therapy remains limited by a lack of clinical experience, and multi-target CAR-T cells only address antigen loss. CAR-based cell therapies still need to address issues such as effective cell generation, tumor infiltration, and cytotoxicity.
Sino Biological, the world’s leading supplier of bioreagents and CRO services for biopharmaceutical research, offers comprehensive solutions for CAR-T and CAR-NK cell therapy development. Our reagents and services support our clients through the whole developmental process, from early target discovery to preclinical research and development.
References
- Maakaron, J., et al. BMJ. 378:e068956 (2022).
- Pan, K., et al.J Exp Clin Cancer Res41, 119 (2022).
- Tokarew, N., et al. Br J Cancer 120, 26–37 (2019).
- Laskowski, T., et al. Nat Rev Cancer 22, 557–575 (2022).
- Zhang, L., et al. Biomarker Res 10, 12 (2022).
- Barros, L. R. C., et al. Cancers, 14, 2667 (2022).
- Wang, Sh., et al. eBiom. 76, 103873 (2022).
- Qin, V. M., et al.Cancers.13(3):404 (2021).
- Su, S., et al. Cells. 11(10):1652 (2022).
- Safarzadeh Kozani, P., et al. Mol Cancer Ther 20 (7): 1223–1233(2021).