Chimeric antigen receptor (CAR) T Cell therapy has emerged as a promising immunotherapeutic approach to treat blood cancers, even leading to long-lasting remission for some advanced cases. The FDA has approved six CAR T Cell therapies to treat some forms of lymphoma, leukemia, and multiple myeloma.
T cells, a component of the immune system, carry out the cytotoxic mechanisms of the anti-tumor immune response, which means that they seek out, attack, and kill cancer cells. T cell receptors (TCR) recognize proteins, called antigens , on the surface of cancer cells, and this recognition activates anti-cancer immune pathways. Tumors can evade the immune system when TCRs do not adequately recognize antigens on cancer cells.
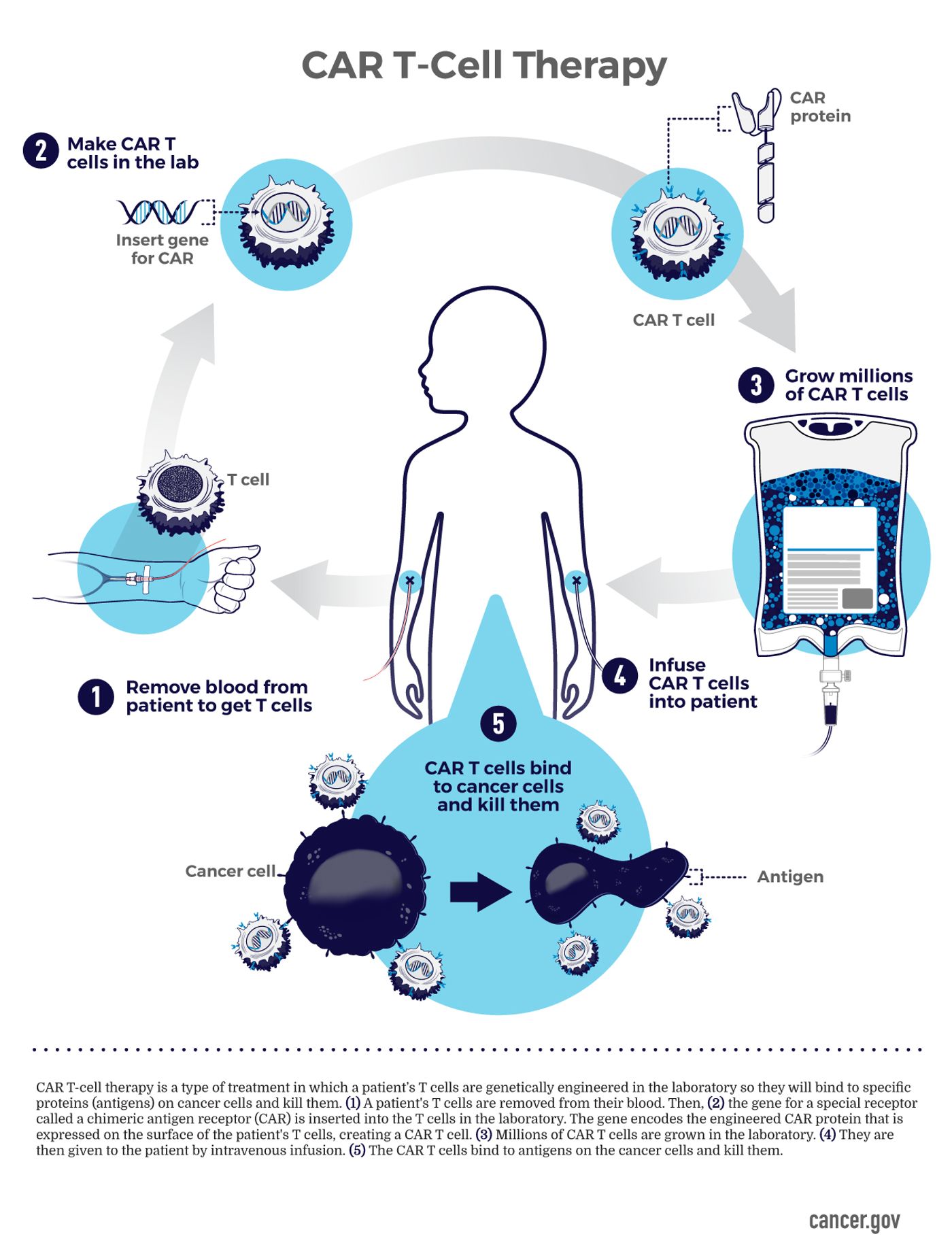
CAR T cell therapies consist of specially engineered T cells programmed to recognize cancer and promote immune activation and subsequent cancer cell death. To generate CAR T cells, doctors harvest a patient’s T cells by drawing blood. Then, specialized technicians modify the T cells in a laboratory, resulting in a TCR primed to recognize the patient’s cancer. The CAR T cells are then expanded so that doctors can return large numbers of highly effective immune cells to the patient.
While CAR T cell methodology has led to cures in hard-to-treat cancers, only about half, or fewer, patients treated with CAR T cells experience long-term remission. Thus, identifying mechanisms behind the relapse of CAR T cell-treated cancers is a high priority among cancer researchers. A study published in Cancer Discovery has uncovered a potential explanation for the reduced remission rates seen in CAR T cell-treated non-Hodgkin lymphoma (NHL).
One CAR T cell modality used to treat NHL targets CD19, a protein present on lymphoma cells. This treatment is effective in less than 40% of patients. The researchers investigated the genetic landscape of CAR T cells following infusion. Patients provided pre- and post-infusion samples, which researchers analyzed using single-cell sequencing. The study included 17 patients, 13 responded favorably, and four responded poorly.
The researchers found that non-responding patients exhibited a different exhaustion profile than those who responded. They identified one marker significantly associated with poor CAR T cell response: TIGIT (which stands for “T cell immunoreceptor with immunoglobulin and ITIM domain”). The association between poor response and TIGIT suggests it is a viable target for cancer immunotherapy.
The study also included a pre-clinical component where a mouse model of human NHL was used to assess the potential impact of TIGIT blockade. The researchers found that blocking TIGIT, in combination with CAR T cells, improved the efficacy of the CAR T cell treatment.
Sources: Nature, Blood Advances, Cancer Discovery, Curr Opinions Oncol, JITC, NCI Visuals Online