There are foods we like, their foods we could eat based on situations and their foods we cannot stand. This adverse reaction to certain foods when encountering food due to adverse post ingestion consequences is called Conditioned Taste Aversion (CTA). This learned association is an evolutionary defense/survival mechanism to help mammals avoid ingestion of toxic foods. CTA is always confused to be an example of Pavlovian conditioning, but it is more an operant conditioning, where the avoidance of food is learned as previous experience led to a gastrointestinal malaise (GIM). The unusual features of CTA that deviate from traditional learning are
1. Rapid Learning: Only one trial/taste of aversive food it enough to develop CTA.
2. Long -Temporal delay: Even if the food-induced, the adverse effect is after a period, CTA still develops.
3. Non-conscious CTA: acquired without conscious awareness and sometimes food consumption followed by an unrelated gastrointestinal sickness can also cause CTA.
4. CTA is also learned when it is not even associated with food. Like when we eat something, and later we suffer some unrelated adverse side effect, we develop an aversion to that food. For example, chemotherapy patients often become nauseated due to the drugs, but they generally associate it with the food consumed and develop CTA.
5. Generalization: Foods of a similar type will also induce CTA despite one’s ability to discriminate the food types. This condition causes the adverse tumor anorexia in cancer patients, as they perceive that all foods cause nausea and avoid food in general.
Dr. John Garcia first observed the CTA in animals in 1950, when he found that the laboratory animals post-exposure to radiation-developed avoidance to foods presented before the radiation. He later investigated this effect in a more systematic manner, which is sometimes referred to as the Garcia effect. Watch the video to know more about Garcia’s work.
CTA is different from the taste avoidance learning (TAL). TAL is another food defense mechanism developed when ingestion of a particular food is paired with a painful external stimulus like a shock when eating the food. I both cases, the associated food is avoided. However, previous studies showed that although identical in food intake, CTA and TAL have different influences on palatability. TAL does not affect palatability. Work done by Joe et al., in 2017 with lactose malabsorption has provided additional evidence to differentiate CTA and TAL. Additionally, CTA is more due to taste cues, and TAL is due to the audiovisual cues.
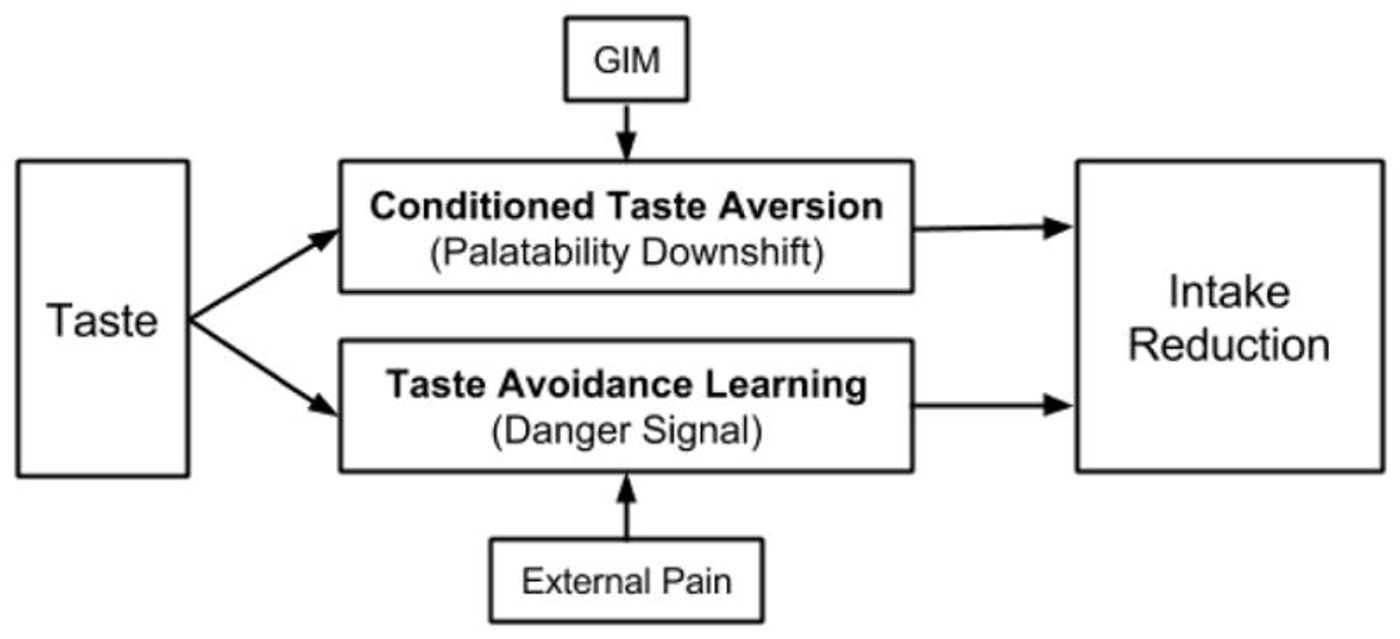
Image Credit: Lin et al., 2014
See the image below to understand how our brain perceives the taste information.

Image credit: Washington Education
Work done by researchers from the Howard Hughes Medical Institute published in the Journal of Neuroscience in 2015 has identified a group of calcitonin gene-related peptide (CGRP) expressing neurons within the parabrachial nucleus that mediate the distress response signal and establishes the CTA. Taking this further, Dr. Chen from the same institute published his findings on how these CGRP neurons are crucial for CTA and how they exhibit synaptic plasticity and are activated in response to CTA. The work is published in Neuron on November 21st. The study also demonstrates that silencing the CGRP neurons prevents the CTA manifestation.
If we can learn to avoid toxic food, can we also unlearn undesired habits? CTA beyond the natural survival mechanism: “Sensitization Therapy or Aversion therapy,” usually suggested for humans to condition them again smoking or drinking uses CTA. When a deliberate addition of compounds making them sick are introduced whenever subjects indulge in either of the activities, resulted in them being repulsed to smoking or drinking. This effect is first shown by Nicolaus and colleagues in 1983 for controlling cow predation of farm eggs. A study by Smith and Frawley in 1990 first tested the therapy for alcohol abstinence effect in humans. Video shows about the aversion therapy.