
Prostate cancer (PC) is the second most commonly diagnosed cancer in men, with an estimated 1.4 million diagnoses worldwide in 2020.1
Systemic therapy, based on androgen deprivation, is standard primary treatment for advanced PC. Despite adequate therapy, the disease eventually progresses to castration-resistant prostate cancer (CRPC).2
In metastatic CRPC, standard first-line therapy combines androgen deprivation therapy (ADT) with therapies targeting the androgen-receptor (AR) pathway, including abiraterone, apalutamide, and enzalutamide.3
In CRPC, in addition to hormone resistance, neuroendocrine differentiation (NED) is an alternative AR-independent mechanism of resistance to cancer therapeutics, especially androgen deprivation agents. This resistance manifests, after exposure to multiple treatments, by a histological change from an adenocarcinoma to a neuroendocrine histology.
Neuroendocrine prostate cancer (NEPC), which includes both pure small-cell carcinoma and mixed adenocarcinoma-neuroendocrine tumors, is characterized by a diminished secretion of prostate-specific antigen (PSA), often accompanied by expression of neuroendocrine markers, such as chromogranin A (CgA), synaptophysin, and neuron specific enolase (NSE).
Small-cell PC, an extremely aggressive histological variant of PC, is extremely rare: occurring in fewer than 1% of men with untreated PC. While NEPC is rarely diagnosed de novo, about 10-17% of patients with metastatic CRPC have been reported to progress with treatment emergent NEPC when treated with new hormonal agents.4
Chromogranin A (CgA) is the main constituent of secretory granules of neuroendocrine cells. In these cells, CgA regulates the storage and secretion of hormones and neuropeptides and is a precursor to biologically active peptides.5
Elevated levels of CgA in men with PC may suggest the emergence of neuroendocrine tumor cells or progression of pre-existing neuroendocrine tumors or sub-populations. Transdifferentiated NEPC cells—like normal neuroendocrine cells—produce, store, and secrete CgA.6
The value of CgA as a prognostic and therapy-predictive biomarker in the localized and mCRPC settings has been tested and remains highly controvertial.7-13 A recent analysis of serum CgA levels before and after treatment with either radical prostatectomy (RPE), chemotherapy (docetaxel), or hormonal therapy (abiraterone/enzalutamide) was reported. The analysis included 395 men with PC that were divided into 3 cohorts according to treatment: the RPE, DOC, and ABI/ENZA cohorts. Men with localized and hormone-naïve PC were included in the RPE cohort; while those with mCRPC were included in the DOC and ABI/ENZA cohorts.14
CgA levels, at baseline, were approximately 3-fold higher in the DOC and ABI/ENZA cohorts, including men with mCRPC, compared to the RPE cohort, including men with localized PC. The median baseline CgA level was 111.1 ng/mL in the DOC cohort and 149.9 ng/mL in the ABI/ENZA cohort. This is in line with previous observations that neuroendocrine differentiation status significantly progresses during ADT and is associated with an increase in serum CgA levels. (Figure 1)
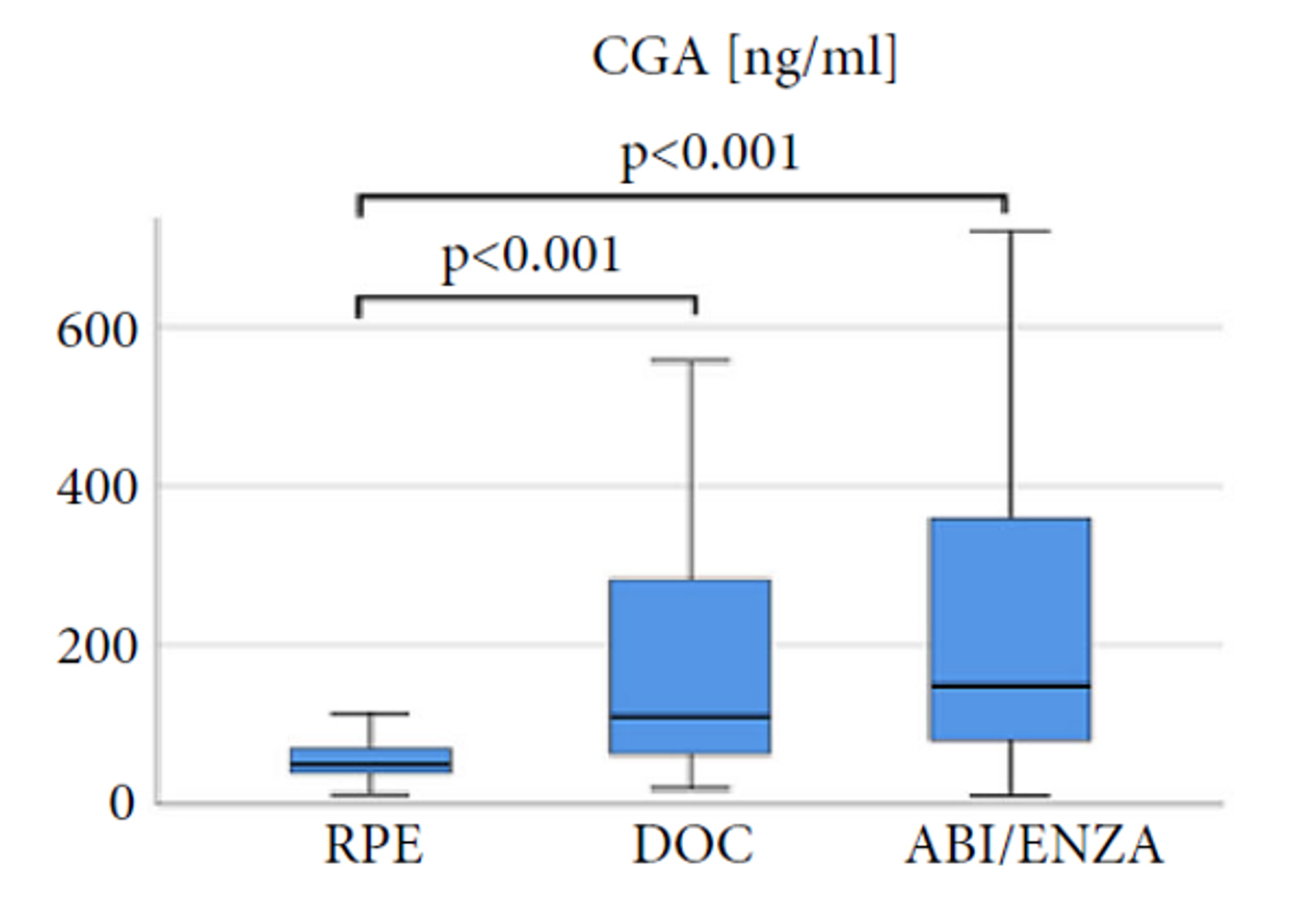
Figure 1: Baseline chromogranin A (CgA) levels before radical prostatectomy (RPE), in men with localized prostate cancer, and before docetaxel (DOC) or abiraterone (ABI)/enzalutamide (ENZ) treatment, in men with metastatic castration-resistant prostate cancer.
This study also suggests that in men with mCRPC treated with DOC, an increase in CgA levels predicts a poor prognosis. Also, in men with mCRPC treated with ABI/ENZA, CgA levels that increased by 50% of the baseline levels were associated with shorter survival. Baseline CgA values were associated with overall survival (OS) as demonstrated by the Kaplan-Meier curves in Figure 2. In this figure, following thresholds were used for CgA, 168 ng/mL in Docetaxel group and 85 ng/mL in the Abi/Enza group.
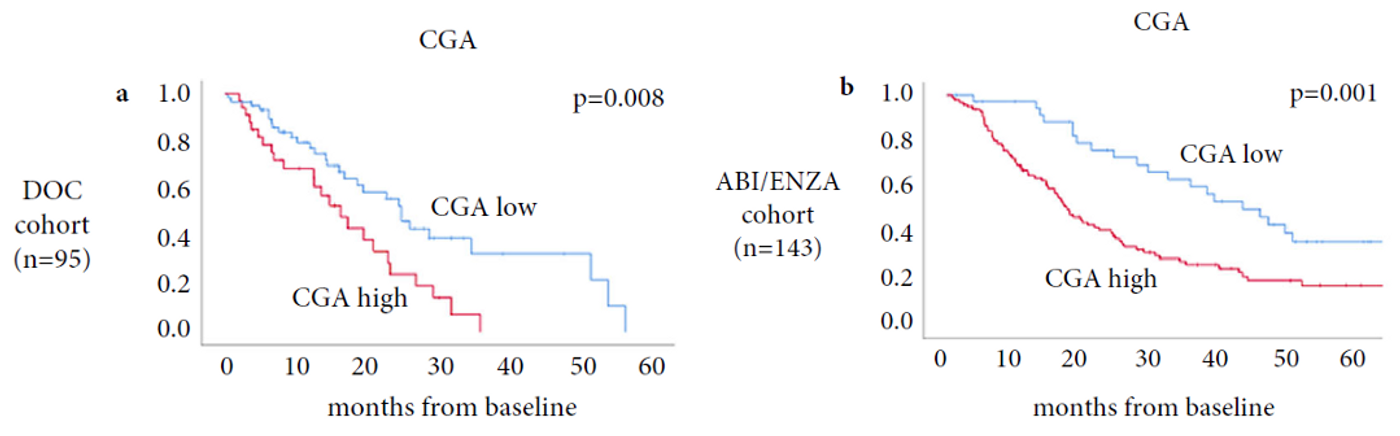
Figure 2: Overall survival curves in the DOC and ABI/ENZA cohorts for baseline values
The analysis of CgA levels before initiating hormonal therapy and those that increase by >20% at 3 month, may provide data to derive an improved prognostic model for men with PC.
A recent systematic analysis of clinical studies that assessed CgA levels suggests that CgA may be a useful biomarker for monitoring disease evolution and for guiding treatment in men with mCRPC.15 (Figure 3)
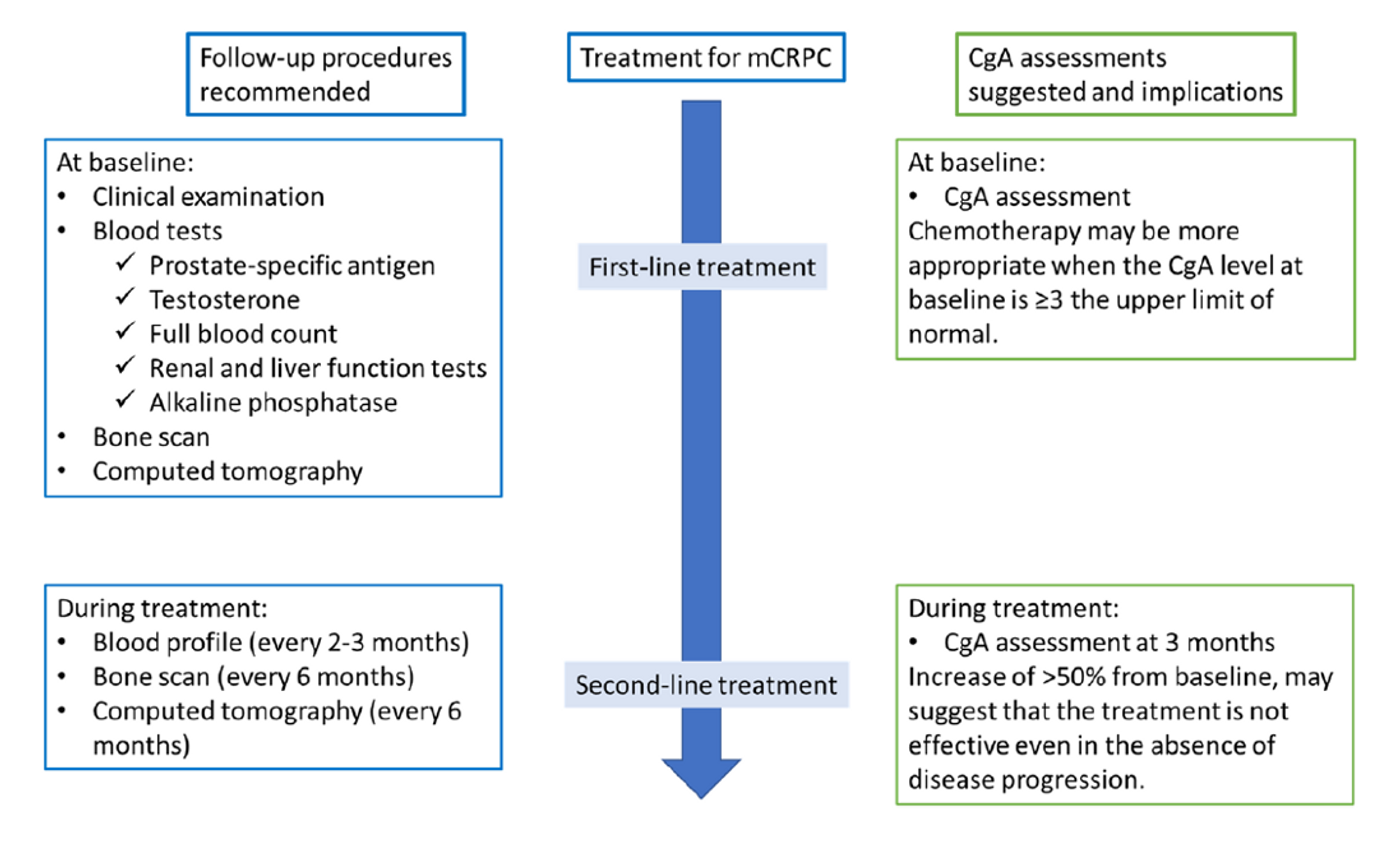
Figure 3: Suggestion of CgA monitoring during treatment sequencing.
In conclusion, the presence or progression of neuroendocrine differentiation is reflected by serum CgA levels. NED significantly progresses during ADT. High baseline CgA levels and increased CgA levels after 3 months of hormonal treatment with Abiraterone or Enzalutamide are significantly associated with shorter overall survival, suggesting NED-related resistance to therapy. Systematic CgA assessments in clinical practice, at baseline and during treatment, may be useful for monitoring disease evolution and assisting physicians with choosing and modifying therapy.
Check out what experts say in this respect HERE and ask your questions HERE.
References
1. https://uroweb.org/guidelines/prostate-cancer/chapter/epidemiology-and-aetiology
2. Kluth LA et al (2014). The hypothalamicpituitary-gonadal axis and prostate cancer:
implication for androgen deprivation therapy. World J Urol 32 (3): 669-676
3. Rozet F et al (2020). Recommandations françaises du Comité de cancérologie de l’AFU –
actualisation 2020-2022 : cancer de la prostate. Assoc Française d’Urologie.
4. Merkens L et al (2022). Aggressive variants of prostate cancer: underlying mechanisms of
neuroendocrine transdifferentiation. J Exp Clin Cancer Res 41:46
5. Laguerre F et al (2020). Chromogranin A in the early steps of the neurosecretory pathway.
IUBMB Life 72:524 – 532
6. Corit A et al (2018). Circulating chromogranin A and its fragments as diagnostic and
prognostic disease markers. Pflugers Arch 470: 199-210
7. Niedworok C et al (2017). Serum chromogranin A as a complementary marker for the
prediction of prostate cancer-specific survival. Pathol Onco Res 23:643-508. Burgio SL et al (2014). Chromogranin A predicts outcome in prostate cancer patients treated
with abiraterone. Endocr Relat Cancer 21: 487-93
9. Heck MM et al (2017). Chromogranin A and neurone-specific enolase serum levels as
predictors of treatment outcome in patients with metastatic castration-resistant prostate
cancer undergoing abiraterone therapy. BJU Int 119: 30-7
10. Fran L et al (2017). Chromogranin A and neurone-specific enolase variations during the first 3
months of abiraterone therapy predict outcomes in patients with metastatic castration-
resistant prostate cancer. BJU Int 120: 226-32
11. Dong B et al (2017). Influence of abiraterone acetate on neuroendocrine differentiation in
chemotherapy-naïve metastatic castration-resistant prostate cancer. Prostate 77: 1373-1380
12. Conteduca V et al (2014). Chromogranin A is a potential prognostic marker in prostate cancer
patients treated with enzalutamide. Prostate 74:1691-1696
13. Giridhar KV et al (2018). Serum chromogranin A-based prognosis in metastatic castration-
resistant prostate cancer. Prostate Cancer Prostatic Dis 21: 431-437
14. Szarvas T et al (2021). Comprehensive analysis of serum chromogranin A and neuron-specific
enolase levels in localized and castration-resistant prostate cancer. BJIU Int 127:44-55
15. Ploussard G et al (2023). Chromogranin A: a useful biomarker in castration-resistant prostate
cancer. WJU 41:361-369
Article number: BMKT001101.1 EN

















































